What can Osteopractic Physical Therapy do to help?
A thorough evaluation of the injured area as well as the knee, hip, pelvis, and lumbar spine will be performed first. Any structural issues, impairments of strength, flexibility, or joint mobility will be identified. A comprehensive evaluation is essential to guide the treatment.
Any dysfunctions in the lumbar spine may be treated first order. Pain in the extremities is modulated through the spine, and therefore, reducing spine pain will also serve to reduce pain in the limbs. This is one of the foundational principles of chiropractic care and why chiropractic manipulation is proven to be an effective pain relieving tool8. Although Osteopractic physical therapists are not chiropractors, they are well trained in spinal manipulative therapy.
Any other joint restrictions at the hip, knee, ankle, or foot will also be addressed with peripheral joint manipulation techniques. It is quite common to see joint restrictions at the ankle and hind foot.
Joint manipulation is then followed by soft tissue treatment. Any areas of of tenderness or poor flexibility will be addressed with various massage techniques. Different techniques may include trigger point release, body tempering (the use of a heavy weighted cylinder to compress and stretch the tissue), and instrument assisted soft tissue massage (scraping and cupping).
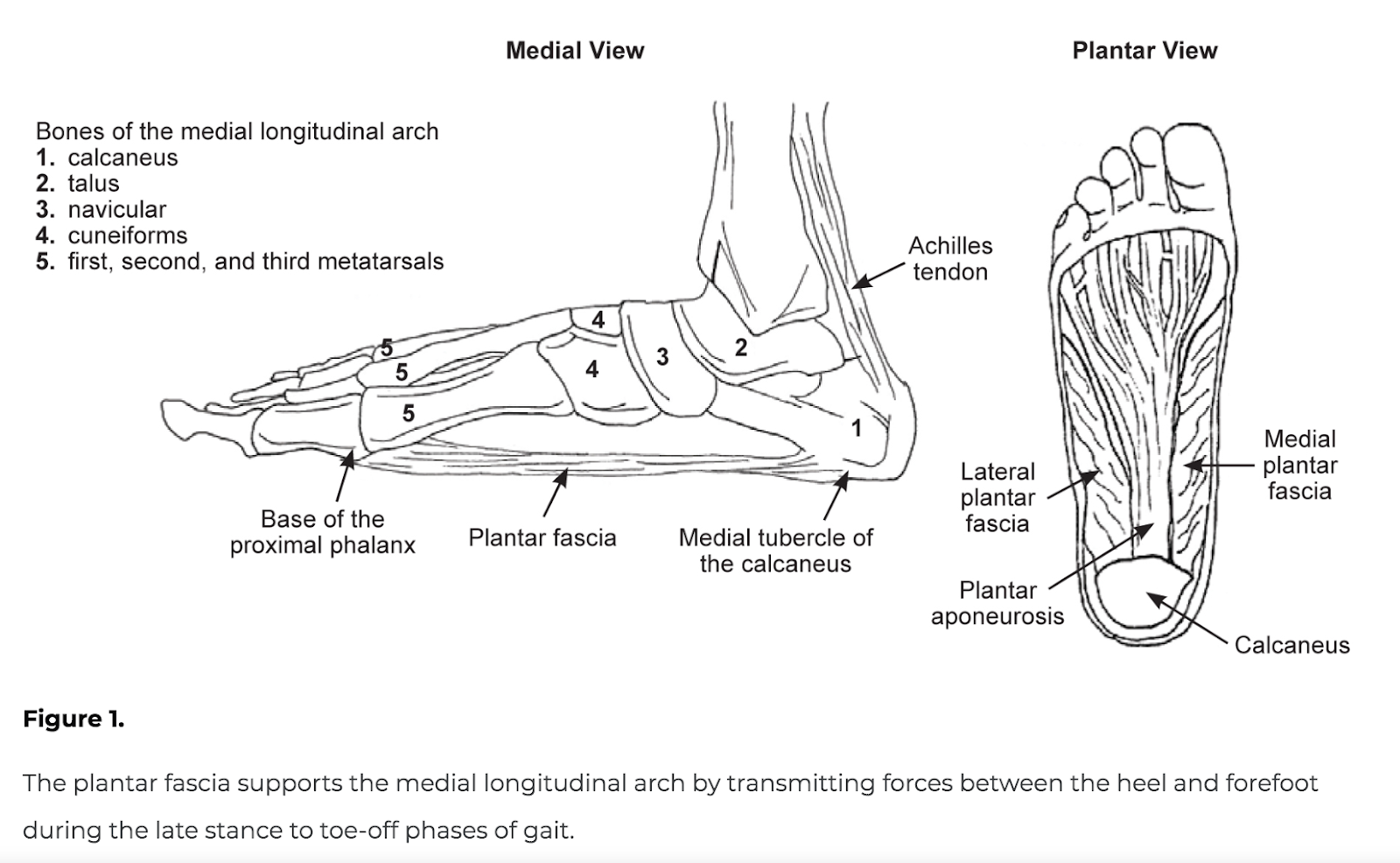
Electrical Dry needling would also be utilized if possible, as this modality has been proven to be extremely effective in the the treatment of PF7. Dry needling is the use of acupuncture needles inserted into areas of tissue dysfunction. The needle can penetrate into areas where fingers tips cannot reach, such as the tissue enthesis of the plantar fascia at the medial calcaneal tubercle. The penetration of a thin needle into the deep tissue layers where the heart of the injury lies serves to stimulate blood flow and facilitate the healing process in a way that no other modality is capable of doing. The use of acupuncture needles is a treatment approach proven to be extremely effective in injury management. Although Osteopractors are not acupuncturists, they are well trained in the use of acupuncture needles to treat injuries of the muscles, tendons, ligaments, joints, and nerves.
Lastly, a well-designed home exercise program along with education regarding self treatment strategies is key to long term success with this injury. Understanding the importance of proper footwear along with active rest and proper exercise is usually the catalyst to full recovery from plantar fasciitis.
In summary, the most effective treatments for any injury include chiropractic care, acupuncture, massage therapy, and physical therapy. The goal of osteopractic physical therapy is to eliminate the need for the consumer to require several different practitioners when they can get all of their needs met in one location.
If you or someone you know is suffering with plantar fasciitis, fear not. Successful, treatment is only a phone call away.